Enhancing the Role of Case Managers to Resolve SDoH
Enhancing the Role of Case Managers to Resolve SDoH

When case managers partner with a structured community-based palliative care (CBPC) solution, they gain a set of “eyes and ears” into the homes of members struggling with a serious illness, resulting in better care coordination and better outcomes for members and their families.
As care for members with a serious illness increasingly shifts to the home setting, case managers welcome an extra level of support to:
- Assess the specific situations and problems associated with clinical/non-clinical issues and social determinants of health (SDoH)
- Coordinate timely solutions that prevent small issues from snowballing into major, costly healthcare events
CBPC provides this level of support, effectively resolving the problems to overcome gaps in care and avoiding unplanned, expensive care. A systemized CBPC , like Turn-Key Health’s Palliative Illness Management (PIM) program, serves as a collaborative partner for case managers, deploying a dedicated palliative care team – primarily nurses and social workers – to engage with members in the home environment and provide a first-hand look at specific situations and problems.
During home visits, these palliative clinicians provide “eyes and ears” to discover what is really going on inside the home – ranging from the problems of food inadequacies and accessing transportation to housing insufficiencies or identifying and addressing other concerns, such as social isolation and depression. Utilizing structured assessments, the CBPC team assesses the issues, provides education and support, initiates referrals to community resources and communicates assessment findings and the plan of care directly with the case manager.
Since the myriad of challenges related to are exponentially magnified for seriously ill members, especially seniors who live alone far away from family and friends, case managers are recognizing the value of the insights gained and support provided by PIM.
Case Examples
Meet Robert
Robert is a 69-year-old man with COPD who lives alone. He was set up to receive his medications from a local big-box store but was unable to get there to pick up his medications. He was stressed by the situation and began “rationing” his medications while trying without success to find someone to drive him to the store. His inability to comply with treatment led to an ER visit and long hospital stays.
Meet Betty
Betty is a 74-year-old woman with lung cancer who lives alone and has no children or family to help her. Her severe mobility issues prevented her from leaving the second floor of her home. While the daughter of her physical therapy aide came twice a week to leave her cooked vegetables, the lack of proper nutrition was beginning to impact Betty’s health status. This led to numerous preventable and unnecessary ED visits.
Optimized, Process-Driven Approach for Resolving SDoH
PIM’s standardized and structured CBPC approach identifies and engages members like Betty and Robert, who are living at home and struggling with multiple clinical and non-clinical issues. These four steps set the foundation for gaining insight into the member and caregivers’ understanding of the illness and medical needs and implementing activities to resolve the issues:
- Engaging with members and caregivers in the home to more accurately identify the scope and intensity of the problems
- Developing a palliative plan of care to address gaps in care and other priority needs
- Coordinating outreach to community resources, such as making contact with neighbors, friends, family members, religious and community organizations that can assist
- Following up to ensure that the problems impacting the member’s day-to-day life and quality of care are resolved
Using structured assessments and methodology, CBPC teams of highly trained professionals develop a trusting relationship with members and their families during home visits and communicate their findings directly to case managers.
For Betty, the CBPC care team assessed the situation and put “Cuisine for Healing” into place so that daily, organic, locally prepared meals were delivered daily to her home. Doing so improved Betty’s nutritional status and reduced her social isolation.
For Robert, the team put a mail delivery service into place for home delivery of his medications that also made it easier to adhere to his medication regimen.
These simple solutions prevented issues related to SDoH from evolving into more costly clinical issues, and resulted in a more compassionate, affordable and sustainable level of care.
The role of case managers working with PIM professionals is enhanced by the addition of greater insights from those involved in the more hands-on aspect of care. Together, they help the “whole person” and overcome gaps in care. PIM addresses SDoH, supports advance care planning, reduces over-medicalization and helps case managers to establish a more robust relationship with members. What’s more, payers can scale these programs across broad and diverse geographic regions to effectively implement this level of engagement throughout the enterprise.
Related Blog Posts

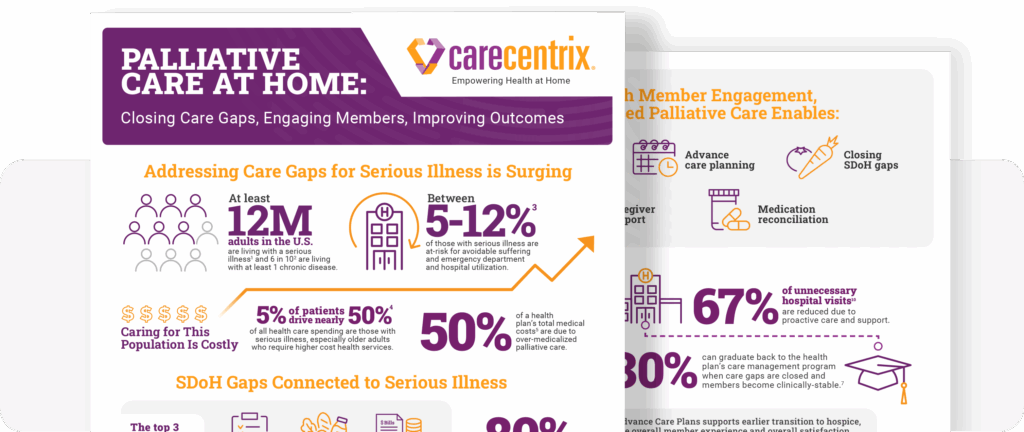
Palliative Care at Home: Closing Gaps, Engaging Members
Supporting members with serious illness can become costly. The need…
Family Caregivers: How Palliative Care Can Help
Facing a serious illness is overwhelming for patients, their family…

Moving Palliative Care from the Hospital to Home
Payors are constantly looking for ways to enhance the member…
