Expanding the Definition of Care Coordination for Members with Serious Illness
Expanding the Definition of Care Coordination for Members with Serious Illness

Addressing clinical and non-clinical issues creates a better patient care experience, promotes improved outcomes and strengthens the medical home.
There’s little doubt that care coordination challenges are especially daunting for plan members who are seriously ill, living at home and struggling with multiple issues on a daily basis. While there is no industry consensus on the definition of care coordination, the Agency for Healthcare Research and Quality (AHRQ) defines care coordination as “… the deliberate organization of patient care activities between two or more participants (including the patient) involved in a patient’s care to facilitate the appropriate delivery of health care services. Organizing care involves the marshalling of personnel and other resources needed to carry out all required patient care activities and is often managed by the exchange of information among participants responsible for different aspects of care.”
This definition of care coordination traditionally refers to issues related to clinical care — direct diagnosis, treatment or testing, and reporting and documenting care back to the medical home.
There is growing recognition among health care providers and payers of the need to address the often overlooked non-clinical issues that can impact care quality. These issues are often associated with social determinants of health, such as food insecurity, low health literacy, or need for transportation to fill prescriptions or attend physician appointments. Left unaddressed, they represent serious gaps in care that frequently lead to unplanned care and poor health outcomes.
Members with serious or advanced illness frequently face multiple challenges to care coordination:
- What follow-up appointments do I need to schedule? Is there a transportation service that I can use?
- How do I get equipment that may be needed for my care?
- Who is going to help me manage my care at home so I don’t return to the hospital?
- How do I see my doctor or obtain my prescriptions if I can’t drive?
- What if my symptoms get worse?
- Can I get food delivered – or who will do the cooking?
Achieving this level of coordination for both clinical and non-clinical issues is a key focus of community-based palliative care (CBPC) programs. Today, a growing number of health plans are partnering with specialized CBPC solutions to provide a process-driven, systemized approach to closing these gaps in care, both clinical and non-clinical. Thankfully, these innovative programs are now available, many of which are provided by highly skilled nurses and social workers. In the absence of CBPC, members would have a diminished care experience and less-than-optimal outcomes including hospital readmissions or over-medicalized care.
In fact, the introduction of optimized care coordination also provides support to treating physicians who understand the need for these services and appreciate CBPC clinician support to fill the gaps. By assisting physicians and relieving them of the challenges associated with clinical and non-clinical care coordination, this approach enhances their efforts to lead the medical home, improve member outcomes and streamline the care experience.
An independent research study published in the April 2019 issue of the Journal of Palliative Medicine highlights an approach that utilizes systemized, structured methodologies to guide the palliative care clinician team—primarily nurses and social workers practicing at the top of their licenses. The study articulates how this approach results in more compassionate, affordable and sustainable high-quality care, reduced utilization and medical costs.
Care Coordination Support for the Primary Care Physician
The physician-patient relationship is the keystone of care, and our Palliative Illness Management (PIM) solution is designed to enhance member and physician engagement. Our approach keeps the physician/patient relationship at the center of the care and delivers support through our PIM clinicians and social workers. They help to scale constrained medical resources by increasing the reach and frequency of care in order to provide the needed insights into how the member and caregiver are managing at home.
The PIM team assesses the individual’s needs and wishes, develops and implements a person-centered care approach and collaborates with the physician, as necessary. They contact the treating physician(s) for any medication or medical management needs and assure that members have follow-up appointments with their primary care team, specialists or other providers.
When medical concerns or other needs arise, the PIM clinical team contacts the member’s physician or care team directly. Some examples are:
- If/when medical evaluation is required
- Change in member status requiring their care provider’s attention
- Complex member/family circumstances including unsafe home conditions
- Identifies gaps in care, including need for prescriptions, orders, referrals or appointments
- Change in code status is needed
- Member wishes to discuss advanced care planning or care goals
- Hospice eligibility evaluation and/or referral
PIM team professionals will also help the member to address food insecurities, transportations challenges or other social determinants of health that impact daily living. Additionally, the team documents member questions regarding treatment options, and outlines their goals to discuss with their physician or provider as appropriate.
Primary Care Physician Communication and Collaboration
Optimizing care coordination and communication protocols with the member, primary care physician and the health plan care management team are vital components for creating an optimal engagement model.
The PIM clinicians develop a trusting relationship with members and their family during home visits, which is challenging to accomplish solely through telephonic-based care. This relationship sets the foundation for gaining insight into the member and caregivers’ understanding of the illness, clinical and medical needs as well as personal values regarding treatment options.
The team extends the reach of the member’s medical providers, while serving as their “eyes and ears” in the member’s home. This provides a unique vantage to assess and address advance care planning, goals of care, symptom management, disease-specific education, medication reconciliation and gaps in care.
Five Positive Impacts on Care Coordination
PIM positively impacts quality improvement, member satisfaction and over-medicalization, with care coordination services that ensure:
1) Easy access to a range of health care services and providers
2) Skillful communications and effective care plan transitions between providers
3) Emphasis upon the total health care needs of the member
4) Clear, simple information that members and caregivers can understand and act upon
5) Reporting and communications with the medical home.
CBPC translates into an extra level of support that enhances quality of life for members — day after day.
Related Blog Posts

Family Caregivers: How Palliative Care Can Help
Facing a serious illness is overwhelming for patients, their family…

Moving Palliative Care from the Hospital to Home
Payors are constantly looking for ways to enhance the member…

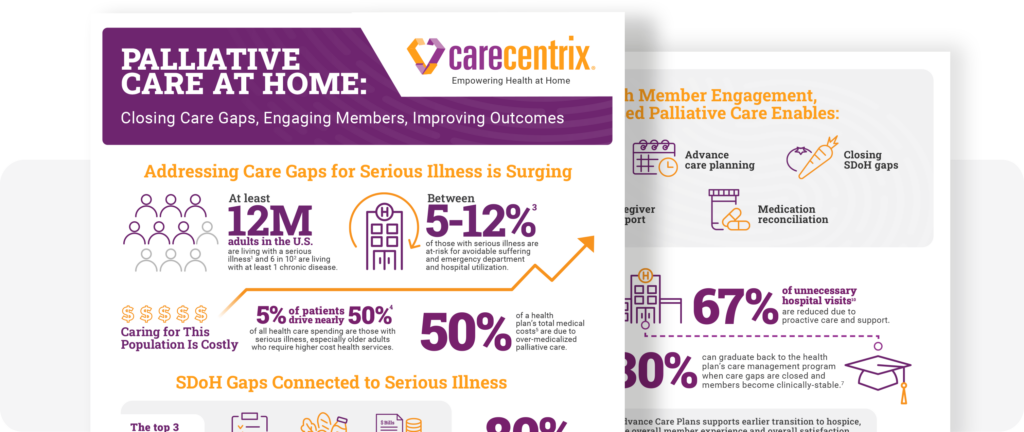
Palliative Care at Home: Closing Gaps, Engaging Members
Supporting members with serious illness can become costly. The need…