23 End of Life Care Buzzwords You Need to Know
23 End of Life Care Buzzwords You Need to Know

We appreciate your interest in this lexicon of new healthcare buzzwords – especially with the growing number of at-risk patients and the associated, escalating costs of care.
Advance Care Planning (ACP)
Making decisions about the care you would want to receive if you become unable to speak for yourself. Provides direction to health care professionals, family and friends regarding care and treatment preferences. Advance care planning is applicable to all adults at all stages of life.
Source: NHPCO
Advance Directives
Also known as Living Wills, Advanced Directives are legal documents that allow you to spell out your decisions about end-of-life care ahead of time, including the use of dialysis and breathing machines, if you want to be resuscitated, if your breathing or heartbeat stops, tube feeding, and organ or tissue donation. Specifies which actions should be taken when the individual can no longer make decisions for themselves based on illness or incapacity.
Source: MedlinePlus
Advanced Illness Management (AIM)
Advanced Illness is defined as “occurring when one or more conditions become serious enough that general health and functioning decline, and treatments begin to lose their impact. This is a process that continues to the end of life.” The goals of AIM are to improve patient and family satisfaction, increase the quality of care, reduce inefficiencies and increase care coordination.
Source: American Hospital Association
Care Transition
The process of a patient moving from one healthcare provider/setting to another. For example, when a patient is discharged from a hospital to a rehabilitation facility.
Source: CMS.gov
Chronic Care Management (CCM) CPT 99490
Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare beneficiaries who have multiple (two or more), significant chronic conditions. In addition to office visits and other face-to-face encounters (billed separately), these services include communication with the patient and other treating health professionals for care coordination (both electronically and by phone), medication management, and being accessible 24 hours a day to patients and any care providers (physicians or other clinical staff). Chronic care management services include at least 20 minutes of clinical staff time directed by a physician or other qualified health care professional, per calendar month, with the following required elements:
- Multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient
- Chronic conditions place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline
- Comprehensive care plan established, implemented, revised, or monitored
Source: CMS.gov
Community-Based Palliative Care
The various care models designed to meet the physical, emotional and spiritual needs of patients with advanced illnesses and their families, outside of a hospital setting.
Source: NHPCO
Complex Care Management
A set of activities designed to more effectively assist patients and their caregivers in managing medical conditions and co-occurring psycho-social factors.
Source: Center for Excellence in Primary Care
Coordinated Care
Coordinated care is the deliberate organization of patient care activities between two or more participants (including the patient) involved in a patient’s care to facilitate the appropriate delivery of healthcare services.
Source: National Center for Biotechnology Information
Extensivist Medicine
Extensivist Medicine is a relatively new area of medicine that focuses on high-risk patient care. An Extensivist Physician is a primary care physician – either an Internal Medicine or Family Medicine physician, who provides comprehensive and coordinated care to patients with multiple complex medical issues.
Source: Health-e-Care
Fifth Vital Sign
The fifth vital sign is the assessment of pain. The four vital signs are blood pressure, body temperature, breathing rate, and pulse. In some care settings, the pain management scale may be used as a ‘fifth’ vital sign, thus leading to the prescription of opioids based on pain symptoms.
Pain is measured on a pain scale based on subjective patient reporting and may be unreliable. Some studies show that recording pain routinely may not change management.
Sources: Everest College and American Pain Society
Healthcare Ecosystem
The healthcare system is now better understood as an ecosystem of interconnected stakeholders, each charged with a mission to improve the quality of care while lowering its cost. To ensure patient safety and quality care while realizing savings, these stakeholders are building new relationships — often outside the four walls of the hospital. These relationships include provider-payer relationship, provider-pharmacist collaboration, medical device manufacturers-clinician communication, employer/payer relationship, and the consumer relationship across all stakeholders.
Source: Beckers Hospital Review
Inappropriate Death
An inappropriate death is the result of care that did not benefit the patient as a whole.
Advanced medical technology has created uncertainty about what interventions are appropriate or potentially beneficial for members with advanced illness. This includes technologies such as dialysis, mechanical ventilation, ventricular assist devices, and parenteral nutrition which make it possible to sustain life.
Given the risk of Non-beneficial Treatment (NBT), however, healthcare providers must balance the potential benefits of medical treatment against the effects on quality of life for the individual, and whether such treatment is consistent with the patient’s personal values and beliefs.
Intensivist
A board-certified physician who provides special care for critically ill patients. Also known as a critical care physician, the Intensivist has advanced training and experience in treating this complex type of patient.
Source: UMass Memorial Health Care
Life Limiting Condition
An illness that leads to death as a direct consequence. Such illnesses may include but are not limited to, cancer, heart disease, chronic obstructive pulmonary disease, dementia, heart failure, neurodegenerative disease, and chronic liver disease.
Source: PCC4U
Non-beneficial Treatment (NBT)
NBT refers to the overtreatment of patients with advanced illnesses, as described in the terms Over-medicalized Care, Over-medicalized Death, and Inappropriate Death.
It is broadly defined as any treatment, procedure or test administered to patients who are naturally dying that will not make a difference to their survival, will probably impair their remaining quality of life, can potentially cause them pain or prolonged suffering, or leave them in a worse state of health than they were.
NBT may prolong life, but at a high cost in terms of social and economic burdens that translate into significant strains on members and their families. These individuals often suffer through unnecessary, even harmful treatments despite overriding expert opinion that, when patients have a terminal illness, at some point more disease treatment does not equal better care.
Source: aci.health.nsw.gov.au
Not Taken Under Care (NTUC)
“Not Taken Under Care” is a hospice term to describe those people who were referred to hospice, but have not been taken care by the hospice team because they do not meet the criteria as defined by CMS. This includes an MD and the hospice MD certification that the person is terminally ill (expected to live 6 months or less), the person does not forego curative treatment (acceptance of palliative care (for comfort) instead of care to cure the illness) or does not sign an agreement choosing hospice care instead of other Medicare-covered treatments for the terminal illness.
Source: NAHC.org
Over-medicalized Care
Over-medicalized care is unnecessary or unwanted interventions that prolong life but diminish patient/caregiver satisfaction with care, such as more days spent in ICU.
A retrospective analysis of outcomes found that, among more than 1.5 million Medicare recipients, treatment in the ICU – which may involve breathing machines, feeding tubes and arm restraints to prevent accidental dislodgment of the various tubes and catheters — was not associated with a survival advantage in patients hospitalized for acute myocardial infarction, COPD or heart failure exacerbations.
Sources: NYTimes and MedPageToday
Over-medicalized Death
This occurs when treatments and technologies are used by default, even when they are unlikely to help the patient. By the time patients are approaching the end, they are often too weak or disabled to express their preferences.
- Chemotherapy for cancer patients within 14 days of death
- Unplanned hospitalization within 30 days of death
- More than one emergency department (ED) visit within 30 days of death
- ICU admission within 30 days of death; or
- Life-sustaining treatment within 30 days of death
This occurs when treatments and technologies are used by default, even when they are unlikely to help the patient. By the time patients are approaching the end, they are often too weak or disabled to express their preferences. In fact, 80 percent of Americans would prefer to die at home, but only 20 percent achieve this wish.
Sources: SOA.org and NYTimes
Palliative Care
Specialized care for members with an advanced illness that provides relief from symptoms and stress, medication management, offers care coordination and other support that may have gone missing from traditional models. The goal is to improve quality of life for both the patient and the family.
Palliative Extensivist™ (PE™)
A Palliative Extensivists™, such as a specially trained nurses, social workers or other clinicians, extend their scope of practice outside the hospital and into the home or other settings. These community-based, specially trained Palliative Extensivists™ are experts at leading sensitive discussions with patients and families regarding goals of treatment. They are resources who are available and affordable, allowing payers to increase the scope and frequency of touching individual patient lives and scale their programs for larger populations.
These professionals aim to help people with chronic illness keep patients healthier outside the hospital. The goal is that such regular, routine visits could help keep patients out of the emergency room, avoid hospitalizations or readmissions, and ICU stays.
Palliative Illness Management™ (PIM™)
New, innovative model offers sophisticated predictive analytics to identify at-risk health plan members who will benefit from an additional layer of in-home, psycho-social support provided by a specialized palliative care program. To engage with these patients and their family caregivers, PIM™ deploys community-based palliative care teams led by Palliative Extensivists™ (PEs), including local, specially trained nurses and clinical social workers.
Source: Turn-Key Health
Population Health
Population health is defined as the health outcomes of a group of individuals, including the distribution of such outcomes within the group. These groups are often geographic populations such as nations or communities, but can also be other groups such as employees, ethnic groups, disabled persons, prisoners, or any other defined group.
Source: IHI.org
Pre-Hospice
Pre-hospice typically refers to those people who are seriously ill and may not yet qualify for hospice services or are not ready for hospice. There are services which are sometimes billable to health plans, including evaluation, consultation and education, and support services. Service levels are usually less intense than those associated with end-of-life care and do not apply to the hospice benefit limit. When compared to hospice care, patients in a pre-hospice program can continue to get curative care and are not required to have a prognosis of six months or less to live.
Sources: NAHC.org and NPR.org
Related Blog Posts

Family Caregivers: How Palliative Care Can Help
Facing a serious illness is overwhelming for patients, their family…

Moving Palliative Care from the Hospital to Home
Payors are constantly looking for ways to enhance the member…

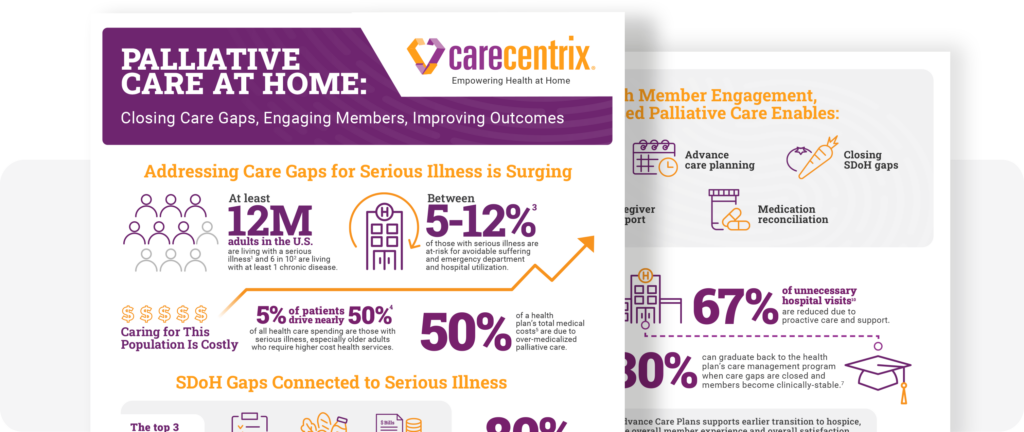
Palliative Care at Home: Closing Gaps, Engaging Members
Supporting members with serious illness can become costly. The need…