Palliative Care Clinicians Improve Care Coordination
Palliative Care Clinicians Improve Care Coordination

Care coordination involves deliberately organizing patient care activities and sharing information among all of the participants concerned with a patient’s care to achieve safer and more effective care. This means that the individual’s needs and preferences are known ahead of time and communicated at the right time and to the right people.
Optimal care coordination is achieved when this information is used to provide care that is not only safe, appropriate and effective, but also meets the personal wishes and treatment preferences of the individual and his or her family.
Palliative care is broadly defined as specialized care for members with serious illness that provides relief from symptoms and stress, and offers medication management and psychosocial support that may have gone missing from traditional models. Provided by specially trained nurses and clinical social workers, palliative care helps to achieve coordinated care using broad approaches, as well as specific care coordination activities:
Examples of broad care coordination approaches include:
- Teamwork
- Care Management
- Medication Management
- Health Information Technology
- Coordination with the Patient-centered Medical Home
Examples of specific care coordination activities include:
- Establishing accountability and agreeing on responsibility
- Communicating/sharing knowledge
- Help with transitions of care
- Assessing patient needs and goals
- Creating a proactive palliative care plan
- Monitoring and follow-up, including changes in patients’ needs
- Supporting patients’ self-management goals
- Linking to community resources
- Monitoring and follow-up, including responding to changes in patients’ needs
- Working to align resources with patient and population needs.
Importance and Value of Care Coordination
The Institute of Medicine identifies care coordination as a key strategy that has the potential to improve the effectiveness, safety and efficiency of the American healthcare system. Well-designed, targeted care coordination that is delivered to the right people can improve outcomes for everyone: patients, provider and payers.
The importance of overcoming barriers and obstacles to care coordination is clear:
Current healthcare systems are often disjointed, and processes vary among and between primary care sites and specialty sites.
Patients are often unclear about why they are being referred from primary care to a specialist, how to make appointments, and what to do after seeing a specialist.
Specialists do not consistently receive clear reasons for the referral or adequate information on tests that have already been done. Primary care physicians do not often receive information about what happened in a referral visit.
Referral staff deal with many different processes and lost information, which means that care is less efficient.
Palliative care places emphasis on advance care planning and draws upon clinician expertise in conducting sensitive conversations that better align treatment options with personal goals of care. Enhanced care coordination results from getting patients and caregivers information on the types of treatments that are available, helping them to decide what treatments match their personal preferences, and completing advance directives that put into writing one’s personal wishes regarding treatment.
Care Coordination Differs from Transitions of Care
Clarification is essential for understanding two key terms: care coordination and transitions of care.
Care Coordination is the deliberate organization of patient care activities among two or more participants (including the patient and/or the family) to facilitate the appropriate delivery of health care services.
Organizing care involves marshalling personnel and other resources to carry out all required patient care activities, which is often managed by the exchange of information among participants responsible for different aspects of the care.
Transitions of Care refer to the movement of patients between health care locations, providers, or different levels of care within the same location as their conditions and care needs change.
Specifically, they can occur:
- Within settings; e.g., primary care to specialty care, or intensive care unit (ICU) to ward.
- Between settings; e.g., hospital to sub-acute care, or ambulatory clinic to senior center.
- Across health states; e.g., curative care to palliative care or hospice, or personal residence to assisted living.
- Between providers; e.g., generalist to a specialist practitioner, or acute care provider to a palliative care specialist.
Care transitions require a set of actions designed to ensure coordination and continuity. They should be based on a comprehensive care plan and the availability of well-trained practitioners who have current information about the patient’s treatment goals, preferences, and health or clinical status. They include logistical arrangements and education of patient and family, as well as coordination among the health professionals involved in the transition. In effect, transitions of care are a subpart of the broader concept of care coordination.
Palliative Care is a Key Strategy
Effective palliative care advances both care coordination and care transitions by supporting patients and caregivers in the identification of issues that impact timely care interventions, avert unnecessary hospitalizations and readmissions, support patient preferences and choices, and avoid duplication of services. Ultimately, this approach uses resources more effectively while improving overall care quality, patient satisfaction and outcomes.
Related Blog Posts

Family Caregivers: How Palliative Care Can Help
Facing a serious illness is overwhelming for patients, their family…

Moving Palliative Care from the Hospital to Home
Payors are constantly looking for ways to enhance the member…

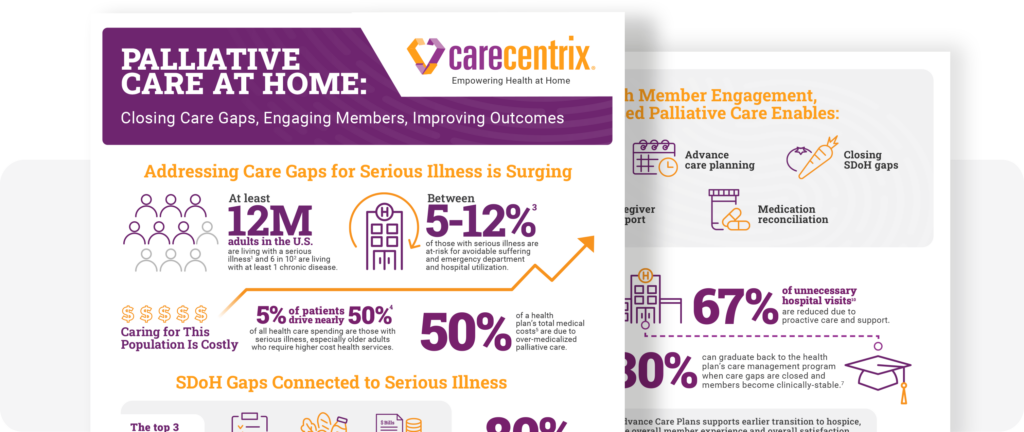
Palliative Care at Home: Closing Gaps, Engaging Members
Supporting members with serious illness can become costly. The need…